Free Cellulite Removal Presentation
Gone for good
A natural way to free cellulite which is stressful to ladies.
Click Here!
Sunday 18 May 2014
Wednesday 14 May 2014
INVASIVE DUCTAL CARCINOMA - Case study
1. SUMMARY
Invasive
ductal carcinoma (IDC) is one of a type of cancerous or malignant tumor which
relates to the breast’s milk ducts and if it is not treated, will be high
possibility to spread to other parts of the breast or body. The symptom of IDC could be having hard
immobilize lump but does not hurt. The
case report regarding one women age 47 who came to the hospital having several
symptoms. The doctor than do clinical
breast examination on her. Based on the
examination, characteristics of the lump on the right breast was noted. Patient was immediately asked to do mammogram
for diagnosis. Mammogram finding shows a
suspicious spiculated lesion and patient was suggested to go for breast ultrasound
as an adjunct to mammogram. Based on the
characteristics of the lesion from mammogram and ultrasound examination,
radiologist concluded that the lesion found in the right breast fall into
BI-RADS category five which is highly suggestive of malignancy. Then, biopsy of the right breast lump was
done and laboratory report confirmed the malignancy. Because of the confirmed malignancy, mastectomy
of the right breast was carried out.
Patient also went other treatment as well such as radiation therapy to
prevent cancerous cell from spreading to another part of the body. Patient should come for checkup annually as a
preventive measure.
2. INTRODUCTION
The
female breast consists of fat, fibrous or connective tissue, glands, 15 to 20
lobes and smaller lobules, and the tiny ducts.
Breast
cancer is called invasive when the cancer spreads outside the membrane of the
lobule or duct into the breast tissue and spread into the lymph nodes in the
armpit area or beyond (invasive breast
cancer: symptoms, treatments, prognosis, 2005). There are two types of invasive breast cancer
which include invasive ductal carcinoma (IDC) and infiltrating (invasive)
lobular carcinoma (ILC). Invasive ductal
carcinoma is the common type of invasive breast cancer which accounts for 80
percent of invasive cancers. While
infiltrating lobular carcinoma only accounts for about 10 percent to 15 percent
of invasive breasts cancers (invasive
breast cancer: symptoms, treatments, prognosis, 2005)
2.1 Definition of Invasive Ductal
Carcinoma (IDC)
Invasive ductal carcinoma is a type
of cancerous or malignant tumor which relates to the breast’s milk ducts and is
able to spread to other parts of the breast or body (breast cancer, 2011). Ducts
are the part of the breast through which milk flow. IDC always starts developing in the breast’s
milk ducts, but breaks out of the duct tubes and invades surrounding breast
tissue. IDC if not treated at an early
stage can invade into the bloodstream or lymphatic system spreading cancer
cells to the other parts of the body (Stephan, 2012).
Invasive ductal carcinoma is more
common to affect a woman as they grow older, yet women at any age may also be
affected. Author from invasive ductal carcinoma (2012) noted
that about two-third of women are 55 or older when they are diagnosed with this
cancer.
2.2 Etiology
From breast cancer: causes (2012) the researcher noted that it is not
clear what causes breast cancer. They
know that when some breast cells begin to grow abnormally, breast cancer will
occur. These cells, rapidly divide more
than healthy cells do and continue to build up, forming a lump or mass (breast cancer: causes, 2012).
However, Chen (2012) stated that
estrogen causes the breast cancer tumor to grow because many breast cancer
cases are sensitive to the hormone estrogen and such cases have estrogen
receptors on the surface of their cells called estrogen receptor-positive
cancer or ER-positive cancer. Certain
women have HER2-positive breast cancer.
HER2 is a gene that help cells grow, divide, and repair themselves and when
cells have too many copies of this gene, they will grow faster (Chen, 2012). Chen (2012) noted that women with
HER2-positive breast cancer have more aggressive disease.
Risk factors of breast cancer
include age and gender, family history, genes, menstrual cycle, alcohol use,
childbirth, hormone replacement therapy, obesity, and radiation (Chen, 2012).
2.3 Sign
and Symptoms
Many
researchers reported that early breast cancer is asymptomatic. However, as the cancer grows, symptoms may
occur. One of these symptoms is breast
lump that is hard, has uneven edges, and does not hurt. Other symptoms are changes in the size and
shape of the breast or nipple and fluid coming from the nipple (Chen,
2012). In advanced breast cancer, the
symptoms include bone pain, breast pain or discomfort, skin ulcers, swelling in
the armpit, and weight loss (Chen, 2012)
3. . CASE REPORT
3.1 Patient History
A woman, 47 years old came to the
hospital with complain of having lump in the right breast and feel discomfort
with it. She is married and has four
children. She never did mammogram before
or any breast surgery. She has second
degree family history of breast cancer which was her aunt from fraternal site. She’s already menopause and not on hormone
replacement therapy (HRT).
She was referred to a breast surgeon
and that breast surgeon did clinical breast examination (CBE) on her. The breast surgeon palpate both breasts to
compare. During palpation she feels the
lump. The lump is in the upper outer
quadrant of the right breast. The lump
felt like a gritty texture and immobility.
Breast surgeon suggested for
clinical follow up and patient was asked to do mammogram as an adjunct to the
physical examination for further evaluation.
3.2 Diagnosis
3.2.1
Mammogram
Mammogram
result reported by Dr Asokan Raman Nair showed a 2 x 1.5 cm lesion in the right
upper outer quadrant which has spiculation.
No microcalcifications seen. No
other focal lesion seen. The left breast
has normal appearance. No enlarged lymph
node seen. The 2 x 1.5 cm speculated
lesion in right upper outer quadrant is suggestive of a carcinoma.
Breast
ultrasound was suggested as an adjunct to mammogram by Dr Asokan Raman Nair to
diagnose whether the lesion is solid or cystic and to confirm the malignancy. Appendix one shows diagnostic imaging report
of mammogram.
3.2.2
Ultrasound
The patient
did the breast ultrasound on the next day.
Ultrasound of the right breast was performed by Dr Vimalah
Rathakrishnan.
Report
showed there are two benign type lymph nodes noted in the right axilla and
these show large fatty hilla. In the
superior lateral quadrant of the right breast, along 10 o’clock line, about 1.5
cm from the areolar margin, there is a 9 mm x 7 mm focal lesion with marked
posterior acoustic shadowing. This
nodule is solid and shows markedly microlobulated margins. There is stromal distortion around this
lesion. Ultrasound features are consistent
with a malignant nodule. The position of
this nodule was marked on the skin. For
the conclusion, there is focal solid nodule in the superior-lateral quadrant of
the right breast along 10 o’clock line has ultrasound features of a focal
malignancy. Appendix two shows
diagnostic imaging report of breast ultrasound.
Biopsy
was suggested for further investigation.
3.2.3
Biopsy
Depend on
the marking that was made during breast ultrasound, the suspected right breast
nodule was biopsies under ultrasound guidance by Dr Vimalah Rathakrishnan. The specimen was sent to histopathology
laboratory for the result.
Histopathology
report came out three days later showed macroscopic appearance of right breast
lump consists of a piece of fibro fatty tissue measures 50x40x30 mm. Cut section showed irregular fibrosis with
small myxoid nodule measures 15x10x15 mm.
Margin is very near about 2 mm.
One section submitted for frozen section. Histology report of frozen section showed
sheets and strands of invasive ductal carcinoma tumor cells with moderate
nuclear pleomorphism and few tubules formation.
Few mitotic figures are seen. The
interpretation for biopsy of this right breast lump is invasive ductal
carcinoma (IDC). Histopathology report
was reported by Dr Norraha Abd Rahman.
Appendix three shows histopathology report of the right breast
lump.
3.3 Patient’s Progress
Patient
was informed about the report where it was confirmed invasive ductal carcinoma
of the right breast. Mastectomy was
suggested by breast surgeon before the extent malignant cells spread to another
part of the body. Patient agreed and
mastectomy was carried out in operation room.
Right mastectomy specimen with axillary contents was sent to
histopathology laboratory to see if there any metastatic carcinoma spread from
the right breast lump. The result showed
right mastectomy specimen with axillary contents residual small focus of ductal
carcinoma in situ component of low grade with lymph nodes metastasis. Margins are free. Appendix four shows histopathology report of
the right mastectomy specimen.
4. DISCUSSION
Appendix five shows
figure 1 – 5 and appendix six shows figure 6 – 11.
Noted
that the risk factors of breast cancer are hormone related risk factor,
lifestyle factor, and genetic risk factor (Rusiecki
et al., 2005). Hormone related
risk factors include age at menarche, parity, age at
first full-term pregnancy, breastfeeding history, menopausal status, and age at
menopause. Lifestyle factor is like
alcohol consumption and elevated body mass index. Genetic risk factor is family history. For this patient, some of the risk
factors mentioned can be the cause of breast cancer. Mentioned earlier that patient already
menopause and according to Henderson (2006) most breast cancer occur during the
postmenopausal years. Another factor
that is important is family history.
Although patient doesn’t have family history of breast cancer in a first-degree
relative who is mother, sister, or daughter, but she has family history of
breast cancer in a second-degree relative which was her aunt. Park et al. (2008) noted studies have shown
that having a history of breast cancer was positively correlated with a higher
perceived risk of breast cancer.
Before
proceeding to mammogram, health professional, breast surgeon will do clinical
breast examination (CBE) on patient first.
Mayer, Batur, and Moore (2010) mentioned that the range of cancers detected
by CBE but not by mammography was three percent to 45 percent. The surgeon
examined patient’s breast for any abnormalities in size or shape and changes in
the skin of the breasts or nipple. Then,
she gently palpate the breasts using the pads of the finger. She will check the location of any lump and
whether the lump is attached to the skin or situated deeper in the tissue. Other than that, is to examine on the axillae
and chest wall for lymph nodes. According
to radiologist, Dr Asokan (personal communication, May 02, 2013), if there is
present of lymph nodes noted, patient is in high risk for breast cancer. However lymph node is usually very tiny and
difficult to detect. If the surgeon can feel
the lymph node, that means the lymph node has already grown larger, probably
patient already have breast cancer and the cancer had already spread to the
lymph node. As for this patient, the
surgeon cannot detect any large lymph node during palpation but there was
suspicious lump felt at the outer upper region of the right breast. The surgeon examined the character of this
lump and found out that the lump was gritty in texture and immobilized. According to Mayer, Batur, and Moore (2010),
characteristic of lump that suggest cancer through palpation include,
immobility, an irregular border, a hard or gritty texture, and a size greater
than two centimeter.
For this
patient, mammogram was recommended for her.
This is because mammography is the gold standard imaging procedure for
detection of early cancer and patient is already 47 years old and had never
done mammogram before. This patient
should have done mammogram examination seven years ago when she turned 40 years
old. Mammogram is recommended for
patient age 40 and above because patient age below 40 tend to have very dense
breast tissue which make mammograms image difficult to interpret. However for patients who are at high risk for
developing breast cancer such as patient with a strong family history of breast
cancer, screening from age 30 is recommended (mammograms in special circumstances, 2013).
Four
standard images had been taken. They are
right cranio caudal (cc) view, left cranio caudal (cc) view, right medio
lateral obliques (MLO) view, and left medio lateral obliques (MLO) view. Because there was a suspicious appearance
found on the right breast, radiologist asked for an additional view which is
magnification view of the right breast on cc view or can be called as right cc
mag as shows in figure five.
Magnification view is very helpful in identifying a true spiculated mass
on a mammogram (Peart, 2005).
According
to Komen (2012), for an assessment of breast density, there are four different
types of breast density shown in the mammography images. These four types are
fatty breast type, some breast density type, more breast density, and dense
breast type. Komen (2012) noted that
these varying breast densities ranging from images of breasts with more fat and
less breast tissue (refer to fatty breast and some breast density types) to
images with less fat and more breast tissue (refer to more breast density and
dense breast types). This patient’s
breast images fall into some breast density type category where images showed
more fat than the breast tissue.
However
the American College of Radiology (ACR) has developed a different way of
describing the breast density. This is
by using Breast Imaging Reporting and Data System (BI-RADS) and this patient’s
breast density fall into BI-RADS two category.
Breast density is classified by BI-RADS into four groups. BI-RADS one, ‘the breast is almost entirely
fat’. BI-RADS one means that fibrous and
glandular tissues makes up less than 25 percent of the breast. BI-RADS two, ‘there are scattered
fibroglandular densities’, means that fibrous and glandular tissue makes up
from 25 to 50 percent of the breast.
BI-RADS three, ‘the breast tissue is heterogeneously dense’ and has more
areas of fibrous and glandular tissue which is from 51 to 75 percent throughout
the breast. Lastly, BI-RADS four, ‘the
breast tissue is extremely dense’ with more than 75 percent fibrous and glandular
tissue made up the breast (mammogram
report – BIRADS, 2013).
There are
four quadrants of the breasts which are upper outer quadrant, upper inner
quadrant, lower outer quadrant, and lower inner quadrant. Cranio caudal (cc) view of the breasts show outer
and inner quadrant as shown in figure one and figure two. Outer quadrant is the portion adjacent to the
armpit area while inner quadrant is the portion adjacent to the chest
wall. Medio lateral oblique (MLO) view
of the breasts shows upper quadrant and lower quadrant. This can be seen in figure three and
four. Portion above the nipple is upper
quadrant while below the nipple is lower quadrant. The suspicious lesion that was reported is seen
on the right breast, in cc view which is located on right outer quadrant of the
breast as shown in figure one. While in
MLO view, it is located on right upper quadrant. This can be seen in figure three. Overall, the lesion is located on upper outer
quadrant of the right breast. Many
researchers stated that from their studies most of the tumor found is at the
upper outer quadrant. Kwong (2003)
mentioned that it is the most common place on the breast to have tumor is the
upper outer quadrant where 36 percent of tumors are found.
Other
than that area, both left and right breasts showed normal appearances. Normal appearance shown means that pectoralis
muscle of both right and left breasts are clear where there is no enlarged
lymph node seen as reported by radiologist.
Adipose tissue also looks normal on both breasts. The ducts and glandular tissue of the left
breast showed normal appearance where there are no spiculated lesions seen as
shown in figure two and four. There are
no microcalcifications seen on both breasts.
According
to Peart (2005) spiculated lesions have a solid central tumor with radiating
structures and ill-defined borders. As
reported by radiologist, Dr Asokan Raman Nair, from mammogram images there is
spiculated lesion in right upper outer quadrant. This lesion measured 2 x 1.5
cm. As show in figure one and figure three
or more clearly in figure five the lesion is white, more enhance than
surrounding tissue and it is stellate in shape.
Stellate means the shape is irregular and looks like a ‘star’. Figure five also shows that the lesion has
ill defined borders and showed that it is a true spiculated lesion because in a
true spiculated lesion the widest diameter of the radiating extensions occurs
at the tumor margins and then tapers distally.
According to radiologist, surrounding the lesions, the breast tissue
showed a little distortion compared to the left breast in figure two where the
appearance of the breast tissue is smooth and no distortion. This abnormal finding suggested of invasive
ductal carcinoma (IDC). Broder and
Lieberman (2005) noted that on mammography IDC can have a wide range of
appearances and in some women it might show slight architectural distortion of
the breast tissue. The masses or lesions
representing IDC usually have any size, irregular shapes, micro-lobulated,
ill-defined or spiculated borders and sometime there is presence of pleomorphic
microcalcifications (Broder & Lieberman, 2005). Breast
cancer (2011) reported that IDC is characterized by a hard lump. The lump will feel harder, firmer, and more
anchored than a benign breast lump. Over
the affected area or the nipple, the skin may be retracted (pulled in) (Breast cancer, 2011). Noted that there is asymmetry of the breast
tissue when comparing right breast (figure one) and left breast (figure two)
because in right breast, the breast tissue posterior and anterior to the
spiculated lesion have been retracted by the lesion itself. This can be seen clearly in magnification
view, figure five.
As a
whole, characteristics of malignant spiculated lesion in mammogram shows
distinct central mass, sharp, dense, fine lines of variable length radiating in
all directions, spicules reaching the skin or muscle may cause localized skin
thickening or skin dimpling, and sometime it is associated with malignant type
calcifications (Peart, 2005). Characteristics
of malignant spiculated lesion are different when compared with benign
characteristic of spiculated lesion. For
benign it shows no solid, dense, or distinct central mass, it may have
translucent oval or circular area at the center. It only have very fine linear densities or
lower density spicules and it is never associated with skin thickening or skin
retraction (Pear, 2005).
Based on
the characteristics of the lesion, radiologist concluded that the lesion found
in the right breast fall into BI-RADS category five which is highly suggestive
of malignancy. BI-RADS is a standard way
of describing mammogram findings which developed by the American College of
Radiology. There are few categories to
describe mammogram findings using BI-RADS.
BI-RADS category one, ‘negative’ used when nothing bad was found and no
significant abnormality to report. BI-RADS
category two, ‘benign finding’ used when radiologist choose to describe a
finding known to be benign such as fibroadenomas. BI-RADS category three, ‘probably benign
finding’ shows finding that have a very good chance of being benign but it is
not proven to be benign, so follow up after six month is recommended. BI-RADS category four, ‘suspicious
abnormality’ shows finding that do not look like cancer but could be cancer and
radiologist always consider biopsy for this category. BI-RADS category five, ‘highly suggestive of
malignancy’ showed finding that looks like cancer and have high chance of being
cancer. For this category, biopsy is
very strongly recommended (mammogram
report – BIRADS, 2013).
Ultrasound
of the right breast was suggested as an adjunct to mammography. This is to confirm the malignancy of the
lesion mentioned in mammogram and to further evaluate the breast lesion and
surrounding breast tissue. Other reason
of doing breast ultrasound is to distinguish between cystic or solid mass.
Anatomy
of the breast shown in ultrasound are skin, three layers of breast tissue,
muscle layer, chest wall, pectoralis muscle, nipple, axillary tail, and ribs
(Lopchinsky, Van, & Kattaron, 2000).
There are three layers of breast tissue in breast ultrasound
images. The first layer is premammary
fat layer which is situated below the skin, second layer called mammary layer,
and third layer where is near to the chest wall is retro mammary layer. Sonographically, breast tissue layers in pre
menopausal women is different from breast tissue layers in post menopausal
women. For this patient, her breast
ultrasound images show breast tissue layers that in postmenopausal women,
figure 10. Figure 11 shows example of
ultrasound image of breast tissue layers that is in premenopausal women.
In
ultrasound, lesions can be divided according to their shape, margins, echo
characteristics, echo texture, and effect on the through transmissions of sound
(Kopans, 1998). Benign lesions usually
are round, oval, or smoothly lobulated. Whereas malignant lesions are irregular
in shape, ill defined, or very lobulated.
Radiologist mentioned that images that are brighter from highly reflective
surfaces are called hyperechoic while areas that are less reflective will
appear as darkened regions are said to be hypoechoic. Areas that have similar echogenicity are said
to be isoechoic to each other. Kopans
(1998) noted that cancers usually always hypoechoic compared to the tissue
surrounding them and they are even lower in echogenicity than fat. Occasionally cancers are isoechoic with the
surrounding tissue. Benign lesions on
the other hand are hyperechoic (Kopans, 1998).
For this
patient, radiologist noted that there was focal solid nodule in the superior
lateral quadrant of the right breast along ten o’clock line, situated about 1.5
cm from the areolar margin and this solid nodule has a feature of a focal
malignancy. This can be seen in figure
seven. Areolar margin is the area
surrounding the nipple. In breast
ultrasound images, radiologist noted that the location of the lesion is
depending on clockwise. For both right
and left breasts, 12 o’clock and six o’clock is always deemed superior and
inferior part of the breast. For right
breast, nine o’clock determine lateral part of the breast while three o’clock
determine medial part of the breast.
Medial part is the one that is near to the chest wall. However for left breast, it is opposite where
nine o’clock determine the medial part of the breast and three o’clock in
lateral part of the breast. As for this
patient, the lesion is situated along ten o’clock line of the right breast
according to radiologist. Ten o’clock is
somewhere between nine and twelve o’clock, so for the right breast where nine
o’clock is consider lateral part and 12 o’clock is superior part, meaning that
the lesion was found in the superior lateral quadrant of the right breast.
The focal
lesion mentioned by radiologist was 9mm x 7mm in size with marked posterior
acoustic shadowing. According to Rudy
(2013), size is not a factor in benign and cancerous breast growth. However, posterior acoustic shadowing was
believed to be a characteristic that defined a malignancy (Kopans, 1998). Figure seven shows the hypoechoic focal
lesion with a posterior acoustic shadowing.
It is noted that the appearance of the lesion is taller than the width. Other
than that it also has an ill defined border, an irregular shape, and
spiculation which appear as a hyperechoic ‘band’ around the mass. This can be seen clearly in figure nine. This nodule is also solid and shows markedly
microlobulated margins according to radiologist as shows in figure eight and
nine. There is also stromal distortion
around the lesion, which can be seen in figure eight and nine. All this characteristics shows suggestion
that the nodule is malignant.
According
to Halls (2010), ultrasound characteristics of benign and malignant solid
breast nodule is different. When that nodule
is benign, ultrasound confirmed absence of malignant findings, hyperechoic or
intense and fibrous tissue like feature, shows two or three macrolobulation, it
is ellipsoid in shape, wider than taller appearance, parallel to the skin, and
sometime it is echogenic and well circumscribed (Halls, 2010). As for potential malignant nodule, ultrasound
characteristics, there will be spiculated outline with alternating echopenic
and echogenic straight lines radiate from the mass, taller than it’s width
because cancers often spread vertically and become taller than the width, shall
also have shadowing because the sound beam fail to pass through the lesion, has
a duct extension pattern because cancer tends to expand toward the nipple
within a duct, and shows microlobulation on the borders (Peart, 2005).
Spiculations
on ultrasound often consist of straight lines that radiate in a perpendicular
fashion from the surface of the breast mass.
Taller-than-wide characteristic suggest of malignancy because one can
conceive that the mass caused by malignancy is aggressive enough to overcome
normal breast tissue barriers and planes, and grow vertically (Halls, 2010). This is because when doing ultrasound,
patient lies supine which make the normal breast tissue planes should have a
horizontal orientation except for this malignant tissue. Microlobulations that are shown on breast
ultrasound indicate the presence of lots of very small lobulations, usually 1
mm to 2 mm on the surface of a solid breast nodule. If the number of microlobulations increase,
the probability that the breast mass is malignant also increases (Halls, 2010). If there is posterior acoustic shadowing on
ultrasound, that’s mean something about the mass or lesions attenuate the sonic
beam strength when compared to surrounding normal tissue. Posterior acoustic shadowing is suspicious
for malignancy because most benign tumors do not usually shadow unless they are
calcified (Halls, 2010).
Previously,
radiologist did mention that there is stromal distortion around the
lesion. Stromal distortion is one of the
abnormal sign on ultrasound and mammogram as well. Stromal is a cell that is connective tissue
cells of any organ that support the function of the parenchymal cells of the
organ (stromal cells, 2013). Other than that, radiologist also mentioned
there are two benign type lymph nodes noted in the right axilla which can be
seen in figure eight and nine. Normal
lymph nodes have the same ultrasound appearance which are hypoechoic, with an
echogenic hilus, and generally oval. While
the malignant lymph nodes are usually hypoechoic without an echogenic hilus,
and round in shape. According to Kopans
(1998), for most of the parts these tumors grow first within the duct
system. As they enlarge they develop the
ability to break out the duct and infiltrate into the periductal stroma and
gain access to the lymphatics and vascular structures, and spread to axillary
and lymph nodes. That is why lymph node
can be seen in ultrasound eventhough they are still benign.
Benign
and malignant lesions of the breast are categorized by the level within the
duct network in which they occur. Some
processes are categorized as if they arose from the cells of the ducts, while
others from the components of the lobules (Kopans, 1998). For this patient, histopathology report
confirmed that the lump or lesion mentioned arose from the cells of the ducts
which give the interpretation of the right breast lump was invasive ductal
carcinoma. Invasive ductal carcinoma is
the most common form of invasive breast cancer and the primary lethal cancer of
the breast (Kopans, 1998). It can be developed
from in situ cancer or develops directly.
The cytologic characteristics of the tumor and its growth pattern
suggest an origin in ductal epithelium.
According to Kopans (1998), many invasive cancers likely obliterate any
residual in situ component, but the in situ clones that are not destroyed by
the invasive cells can continue to grow in and down the ducts, presenting
invasive and in situ cancer in the same lesion.
During a biopsy procedure, radiologist
remove cells or tissues from the suspicious area for the pathologists to
examine more closely in the laboratory.
The pathologists examine the tissue sample under a microscope and assign
a histologic type and tumor grade. Grade
one means that cancers tend to grow the slowest, while grade three shows tumor
spread more aggressively. Other than
that, pathologist also realised the size of the tumor, how closed the cancer is
to the edge of the tissue removed, and whether the tumor invaded blood or
lymphatic vessels.
Invasive ductal carcinoma is treated
through surgery, chemotherapy, hormonal therapy, or radiation therapy. For this patient, she chose surgery.
Mastectomy of the right breast was immediately being carried out where the
entire breast and some or all lymph nodes near the breast were removed. Mastectomy reduces the chances of the cancer
to recurr. Even after undergoing
mastectomy, usually most women with invasive breast cancer will be offered
chemotherapy and hormonal therapy.
Chemotherapy drugs will kill rapidly dividing tumor cells that may be
spreading through the body reducing the risk of the cancer coming back in
another site of the body. Drugs
affecting hormone also kill the tumor cells, which require hormones to grow,
and prevent these cells from spreading or coming back. Radiation therapy is used to rid the body of
any microscopic remnants of the cancer in the area where the original tumor was
found and removed (breast cancer,
2011).
Once the diagnosis and treatment has been
made, patient’s prognosis should be understood.
The prognosis will depend on a few factors and one of these factors is the
type of tumor and the size of the tumor.
The larger the invasive tumor, the worse will be the prognosis. Second factor is lymph nodes, where involving
more lymph nodes, the worse will be the prognosis. Third factor is margin. Margin refers to the distance between the
tumor and the edge of the surgical specimen.
Other factors are hormone receptors, differentiation or grade, lymphatic
invasion, and cancer genes (breast cancer,
2011).
5. CONCLUSION
After
being diagnosed and treated, patient is doing very much better. No matter how, this patient was still being advised
to undergo radiation therapy as a preventive measure. Patient was also reminded to come back within
six month after last mammogram to check on the other breast to make sure
cancerous cell does not spread to that breast.
If the result is normal, she is advisable to come for annual checkup for
clinical breast examination, unilateral mammogram, and ultrasound breasts. The patient may have high tendency to start
having side effects or complications from those cancer treatments. For example, radiation therapy may cause
temporary swelling of the breast (lymphedema), aches, and pains around the area
(breast cancer, 2012).
Now with
advanced technologies, there are a lot of improved treatments that can help
women with breast cancer to survive much longer than before. Even though, breast cancer still can spread
to other parts of the body. Sometimes,
even after the entire tumor has been removed and lymph nodes are found to be
cancer free, cancer still can return and may recurr. That is why many health practitioner will
suggest to all women to go for breast checkup every year so that if there is
cancer cell, we can detect it and treat it before the cancer get worse and
start to spread to other parts of the body.
Women under 40 years old, are recommended to do breast ultrasound while
women above 40 are recommended to do mammogram.
From the result of mammogram and ultrasound, if needed, the radiologist
will suggest for other modalities as an adjunct to previous modality.
Other
approved breast cancer prevention is to take tamoxifen. Tamoxifen is a hormone replacement
therapy. Some or certain patients will
be advised by breast surgeon to take it.
Usually women aged 35 years and older shall be at higher risk. These age group women are those that have
already had one breast removed due to cancer, women with a strong family
history of breast cancer, and women with genes or genetic mutations that increase
their risk potential of breast cancer (breast
cancer, 2012).
Risk
factors like genes and family history cannot be controlled. But we can make a healthy lifestyle
changes. Healthy lifestyle may reduce
the overall chance of getting cancer (breast
cancer, 2012). These include eating
healthy foods and prevent drinking alcohol and smoking.
Unique Features of Mammogram Tube ans X - Ray Spectrum
INTRODUCTION
Mammography
is one of the most demanding radiologic techniques. It requires an excellent spatial resolution
to allow visibility of microcalcifications and good contrast sensitivity to
allow detection of breast tumors. It is
difficult to visualize very small physical changes in breasts with general
x-ray imaging. That is why mammography
equipment was designed differently from general x-ray.
UNIQES FEATURES OF MAMMOGRAM TUBE
Mammography equipment consists of
two major components. They are an x-ray
tube and an image receptor. The x-ray
beam originates at the x-ray tube and transmitted through the breast. A film contained in the image receptor to record
the images from x-ray distribution that passed through the breast tissue.
|
Image
receptor
|
Figure
1. Mammogram
Equipment. Reprinted from Screen-film Mammography Equipment Unit 3, by B.A.
Barnes & X. Ho, n.d., Retrieved from www.santarosa.edu/.../Unit%203%20-%20Mammography. Reprinted with permission.
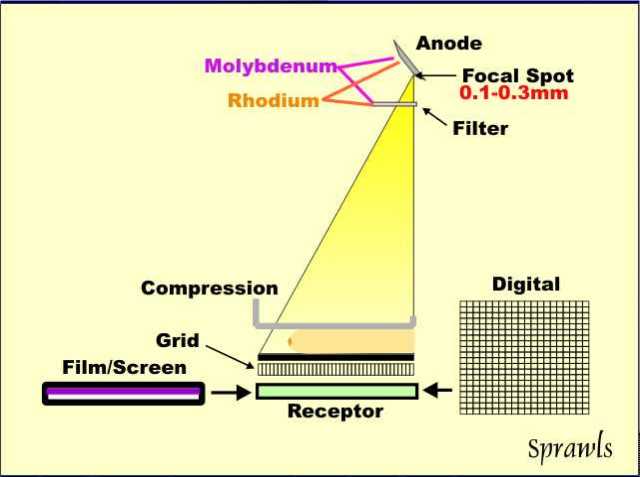
Features of mammogram x-ray tube
that are unique compare to general x-ray tube include x-ray tube anode, target
materials, filament design, filter, focal spots, source-to-image distance, and
object to image receptor distance.
Most x-ray tubes use tungsten as the
anode material, however mammography equipment uses molybdenum and in some
designs, it uses a dual material anode with an additional rhodium track. Molybdenum and rhodium are used because they
produce a characteristic radiation spectrum that is close to optimum for breast
imaging (Sprawls, 1995).
To reduce unnecessary exposure to
the patient, most x-ray machines use aluminum to filter the x-ray beam. Sprawls (1995) mentioned that mammography
uses filters that work on different principle and also used to enhanced
contrast sensitivity. Same as in the
anode, molybdenum is the standard filter material. Some systems allow the operator to select
either the molybdenum or rhodium filter to optimize the spectrum for specific
breast conditions (Sprawls, 1995).
There is also exit window filtration
(Barnes & Ho, n.d.). Instead of
glass, beryllium is used in dedicated mammography tube housing. Noted that glass act as a filter when dealing
with this soft end of the x-ray spectrum, and it filters out photons that would
not provide contrast (Barnes & Ho, n.d.).
Mammographic x-ray tubes typically
have dual filaments in a focusing cups that produces 0.3 and 0.1 mm nominal
focal spot sizes (Barnes & Ho, n.d.).
Meaning x-ray tube for mammography has two selectable focal spots. The spots are smaller compared to other x-ray
procedures because mammogram requires for minimal blurring and good visibility
of detail to see the small calcifications.
The smaller of the two spots is generally used for the magnification
technique (Sprawls, 1995). Magnification
views use a small magnification table which brings the breast closer to the
x-ray source and further away from film plate.
This allows the acquisition of zoomed in images of the region of
interest (special mammography views,
2008).
Other unique component in
mammography tube which is source-to-image distance (SID). SID is the entire distance of the x-ray beam
from the focal spot to the image receptor (Barnes & Ho, n.d.). The greater the distance the less geometric
blurs occur. This affects the focal spot
size which affects the size of the objects being imaged. The larger the SID the larger the field
size. With larger distance of the source
to the image, more beam will be needed to penetrate which then can increased
the heel effect (Barnes & Ho, n.d.).
Other feature is object to image
receptor distance (Barnes & Ho, n.d.).
It is the distance of the object (the breast) to the image receptor. Increase of the object to image receptor
distance will increase magnification of an area of breast tissue. It will increase the resolution and contrast
of the breast image (Barnes & Ho, n.d.).
Figure
2. Principle of Mammogram Tube. Reprinted from Mammography Physics and
Technology for Effective Clinical Imaging, by P. Sprawls, 1995, Retrieved from http://www.sprawls.org/resources/MAMMO/mammo02.jpg. Copyright 1995
by Sprawls Educational Foundation. Reprinted with permission.
{kind=link}
THE X-RAY SPECTRUM
The x-ray spectrum depends on the combination of three factors. First factor is the x-ray tube anode material
(molybdenum or rhodium), second is material used for x-ray beam filtration (molybdenum
or rhodium), and third is the kV which ranging from 24 kV to 32 kV (Sprawls,
1995).
As for x-ray tube anode, most
mammogram unit uses molybdenum anodes.
However, in some systems have a dual-track anode that allows
radiographer or AEC system to select between molybdenum and rhodium.
For
x-ray beam filtration, the material used is also molybdenum but in some systems
they have an alternative rhodium filter that can be selected. According to Sprawls (1995) the molybdenum
filter only should be used with the molybdenum anode. However, the rhodium filter can be used in
combination with both the molybdenum and rhodium anodes.
Figure 3. Factors
Affecting the X-ray Spectrum. Reprinted from Mammography Physics and Technology
for Effective Clinical Imaging, by P. Sprawls, 1995, Retrieved from http://www.sprawls.org/resources/MAMMO/mammo18.jpg.
Copyright 1995 by Sprawls Educational Foundation. Reprinted with permission.
In physics, there are two types of
x-ray radiation produced when electrons hit the x-ray tube anode. They are bremsstrahlung and
characteristic. Bremsstrahlung is in the
form of a broad continuous photon energy spectrum with a maximum energy
determined by the selected kV value (Sprawls, 1995). Characteristic radiation is produced under
certain conditions and is confined to just a few photon energies (Sprawls,
1995).
The photon energies of the
characteristic radiation are determined by the atomic characteristics of the
anode material which varies with the atomic number (Z) of the material. For mammography, molybdenum and rhodium are
materials that produce characteristic x-ray radiation that is near the optimum
energy which is why they are used for the anodes (Sprawls, 1995).
In mammography, the filters used are
based on the ‘k-edge’ principle and it attenuates the radiation above the
k-edge energy of the specific material (Sprawls, 1995).
Figure 4. K-edge
Principle. Reprinted from Mammography Physics and Technology for Effective
Clinical Imaging, by P. Sprawls, 1995, Retrieved from http://www.sprawls.org/resources/MAMMO/mammo28.jpg.
Copyright 1995 by Sprawls Educational Foundation. Reprinted with permission.
Sprawls (1995) noted that with an
atomic number of 42, molybdenum has a k-shell binding energy and its k-edge at energy
of 20 keV and rhodium, with an atomic number of 45 also has a k-shell binding
energy and its k-edge at energy of 23.22 keV.
When molybdenum filter is selected, it attenuates and blocks much of the
bremsstrahlung spectrum above the energy of 20 keV and gives results in the
spectrum that is most often used in mammography which is ‘moly/moly’
anode/filter combination (Sprawls, 1995).
Figure 5. The
Moly/Moly Spectrum. Reprinted from Mammography Physics and Technology for
Effective Clinical Imaging, by P. Sprawls, 1995, Retrieved from http://www.sprawls.org/resources/MAMMO/molymoly.jpg.
Copyright 1995 by Sprawls Educational Foundation. Reprinted with permission.
The k edge boundary is shifted to a
higher energy with the rhodium filter.
So the portion of the bremsstrahlung between 20 keV and 23.22 keV is
added to the x-ray beam. This makes the
beam more penetrating which provides some advantage when taken image of larger
or denser breast (Sprawls, 1995).
Figure 6. The
Moly/Rhodium Spectrum. Reprinted from Mammography Physics and Technology for
Effective Clinical Imaging, by P. Sprawls, 1995, Retrieved from http://www.sprawls.org/resources/MAMMO/molyrho.jpg.
Copyright 1995 by Sprawls Educational Foundation. Reprinted with permission.
Another anode material is
rhodium. Rhodium can be selected to
produce a more penetrating x-ray beam. Rhodium’s
atomic number (Z) is 45 and has principal characteristic radiation at energy of
20.3 keV with a less intense emission at 22.7 keV. Compare to molybdenum which atomic number (Z)
is 42 and principal characteristic energy of 17.6 keV with less intense peak at
19.7 keV (Sprawls, 1995).
The rhodium filter, with a k-edge
cut off at 23.22 keV, is always used with the rhodium anode. The molybdenum filter cannot be used with
rhodium anode because its k-edge cut off from 20 keV upward would attenuate the
rhodium 20.3 keV and 22.7 keV radiations (Sprawls, 1995).
Figure 7. The
Rhodium/Rhodium Spectrum. Reprinted from Mammography Physics and Technology for
Effective Clinical Imaging, by P. Sprawls, 1995, Retrieved from http://www.sprawls.org/resources/MAMMO/rhorho.jpg.
Copyright 1995 by Sprawls Educational Foundation. Reprinted with permission.
Third factor that affect the x-ray
spectrum is kV. Increasing the kV has
two effects on the x-ray beam. First, it
increases the efficiency and output for a specific mAs value and second it
shifts the photon energy spectrum upward so that the beam becomes more
penetrating (Sprawls, 1995). Penetrating
beam reduce contrast sensitivity and it is necessary for dense breast. Therefore compressed breast thickness is the
principal factor that determines the optimum kV (Sprawls, 1995).
Figure 8. KV
Selection for Different Breast Thickness. Reprinted from Mammography Physics
and Technology for Effective Clinical Imaging, by P. Sprawls, 1995, Retrieved from
http://www.sprawls.org/resources/MAMMO/mammo32.jpg. Copyright 1995 by Sprawls
Educational Foundation. Reprinted with permission.
DISCUSSION
According to Sprawls (1995) the
photon energy spectrum of the x-ray beam is one of the most critical factors in
optimizing a procedure with respect to contrast sensitivity and radiation dose. Although many said that anode materials used
in mammogram can only be molybdenum and rhodium, today many researchers do the
study on tungsten as an anode material for mammogram tube to see whether it
still can produce good contrast and low radiation dose.
Between all of the anode materials
used in mammography tube, which are molybdenum, rhodium, and specialized
tungsten, many researchers agree that molybdenum is the best material to be
used because it allows production of low energy spectrums of radiation and only
need low kVp which is 26 to 30 kVp (Barnes & Ho, n.d.).
However, recently there is study done
using tungsten as an anode material with rhodium in mammography and according
to researchers, if the molybdenum x-ray tube digital mammography demonstrated a
30 percent reduction in dose, the introduction of tungsten x-ray tubes with
digital mammography allows even greater reduction in radiation exposure,
without affecting image quality (Smith, Chen, & Semine, 2005).
Another study done from Dance,
Klang, and Sanborg (2000) to compare performance of mammographic x-ray systems
that use different anode/filter combinations for screen film and digital
imaging. For screen film mammography,
result for thicker breasts shows 20 percent improvement in contrast can be
achieved but without reduce radiation dose using molybdenum/rhodium or
rhodium/rhodium, Whereas more than 50
percent of dose saving can be attained but no improvement in contrast using
tungsten/rhodium or rhodium/aluminum spectra.
As in digital mammography, Dance et al. (2000) mentioned that
molybdenum/molybdenum spectrum delivers the lowest dose for a two centimeter
breast, but gives the highest dose for thicker breasts. However tungsten/rhodium or rhodium/aluminum
spectra provide the lowest doses at greater thickness. Researchers concluded that from this study,
molybdenum/molybdenum is the spectrum of choice for all but not for thicker or
most glandular breasts.
CONCLUSION
The most important part of dedicated
equipment in mammography is the x-ray tube.
The tube is designed and constructed uniquely and specifically for
imaging the soft tissue of the breast.
The x-ray machines used for mammograms today designed to produce lower
energy x-rays but improves in image quality and less radiation.
REFERENCES
Barnes, B.A., (n.d.).
Screen-Film Mammography Equipment Unit 3. Retrieved April 27, 2013, from www.santarosa.edu/
Dance, D.R., Klang,
A.T., Sandborg, M., Skinner, C.L., Smith, A.C., & Carlsson, G.A. (2000). Influence of anode/filter material and tube
potential on contrast, signal-to-noise ratio and average absorbed dose in mammography. The British Journal of Radiology, 73 (2000), 1056-1067. Retrieved from
bjr.birjournals.org/content/73/874/1056.full.pdf
Smith, A., Chen, B.,
& Semine, A. (2005). Minimizing Dose in Digital Mammography. Retrieved May 02, 2013, from
www.hologic.com.data/WP_00005_tungsten
Sprawls, P. (1995).
Mammography Physics and Technology for Effective Clinical Imaging. Retrieved April 28, 2013, from
www.sprawls.org/resources/mammo/module.htm
Special
Mammographic Views. (2008). Retrieved April 28, 2013, from www.imaginis.com/mammography/special-mammography-views-spot-c
Subscribe to:
Posts (Atom)